 |
Toll Free 877-238-1437
|
Prostate HDR Mono Brachytherapy
( High Dose Rate (hdr) mono Brachytherapy For Prostate Cancer)
Back to Top1. Introduction
| The two forms of brachytherapy performed today for the treatment of prostate cancer are low dose rate (permanent seed) and High Dose Rate (HDR) brachytherapy. Our physicians did hundreds of permanent seed implants before switching to HDR in 1991 for reasons explained in this page. To date, our center has done over 2,900 HDR brachytherapy implants for prostate cancer. |  |
Back to Top2. Prostate HDR Brachytherapy
HDR Brachytherapy can be used in combination with external beam or as the only treatment method (monotherapy). HDR Brachytherapy is also used as a salvage treatment for men whose cancers have recurred after radical prostatectomy, external beam or permanent seed implantation.Back to TopHDR Brachytherapy is recommended for patients:
- as an alternative to radical prostatectomy, external beam or permanent seeds
- any stage localized disease, Stages T1-T3b
- who have extra-capsular extension, seminal vesicle or perineural involvement
- any PSA value with no evidence of metastatic disease
- any Gleason score
- Prior transurethral resection of the prostate (TURP) with recurrent local disease after radical prostatectomy, external beam or permanent seed implants (salvage)
Back to TopHDR Brachytherapy Procedures
- The physician determines what course of treatment the patient should follow after reviewing the patient's history and recent test results. This is discussed during the consultation. The usual time between consultation and the first implant is 3 to 4 weeks. The day before the implant, the patient comes to the clinic for a pre-op exam and blood test.
- In the OR, the patient is given spinal anesthesia, which numbs the patient from the waist down. The patient's legs are placed in stirrups and the pelvis is positioned by the physician for access to the perineum (the space between the scrotum and anus).
- CET physicians use a non-fixed template technique for placing the treatment catheters, called '"flexiguides'" around and through the prostate. The rubber template has pre-drilled holes arranged in two concentric circles, rather than the square grid arrangement of the fixed template technique. Our physicians feel the circular distribution conforms better to the natural shape of the prostate. The template is held in one hand, while the flexiguides are inserted with the other. Holding the template, rather than having it clamped to the table as in the fixed template technique, allows the physicians to tip and angle the template, resulting in more control over where they can place the flexiguides. Our physicians can flare the flexiguides to encompass any size prostate, perineural or extracapsular disease or seminal vesicle involvement that may be present. This ability to flare the flexiguides enables our physicians to treat larger prostates without having to increase the number of flexiguides, which is 17. The pubic bone can sometimes interfere with the placement of rigid steel needles used in permanent seed implants, but using the non-fixed technique and plastic flexiguides, the pubic bone poses much less of a problem. This means that the patient doesn't have to take pre-implant hormones in order to shrink the gland, a common practice if permanent seeds are used.
- Once the flexiguides are in position, the template is sutured to the perineum to stabilize the implant. A radio-opaque catheter is placed in the bladder for urine drainage and urethral visualization. A rectal catheter is inserted to allow liquid contrast to be inserted into the rectum for radiographic visualization. After a brief stay in the recovery room, the patient is brought to our clinic for radiographic imaging (films and/or CT). Once the images of the implant are obtained, the patient waits for the customized treatment plan to be generated.
- After the physician has approved the treatment plan, the patient is moved into the treatment booth, where the protruding ends of the catheters are connected to transfer tubes, which are in turn connected to the afterloader. Although the patient is alone in the treatment booth, he is constantly monitored via closed circuit TV and intercom. The patient will hear the afterloader click and whir as the source is directed into each of the flexiguides. The Iridium-192 source delivers the radiation dose in about 10 minutes. After the treatment, the source withdraws into the afterloader. The patient is no longer radioactive.
 |
Fig 1: This patient is receiving his treatment. The afterloader is in the lower right corner. | |||
- The patient goes to his hospital room for the overnight stay. He is allowed to roll from side to side, but not sit upright as that would place pressure on the protruding ends of the flexiguides. The next morning, the second treatment is given This second treatment requires much less time because the simulation and treatment planning procedures do not need to be done again. However, a pre-treatment fluoroscopy is done to make certain that the implant hasn't moved during the night. After the second treatment (or third treatment if the patient is having HDR monotherapy), the template and treatment flexiguides are removed. During the removal process, there is some slight bleeding, which is stopped by the nurse or therapist by applying firm pressure to the perineal area with gauze pads. The patient goes back to his hospital room where the nurses make sure that the patient can urinate before going home.
- The second implant is done a week later, following the same procedure as described above.
Back to TopSide Effects
The possible post-HDR acute side effects, usually lasting two to four weeks, are urinary frequency, dysuria, and urinary retention. There may also be some slight rectal irritation. The perineal area will be tender for a few days so activities like bicycle riding that put pressure on this area should be avoided. Medications are prescribed to help alleviate these temporary side effects.Back to Top3D CT Based Dosimetry
One of the great advantages of HDR over permanent seeds is the ability to evaluate the implant in 3-D and know what the doses are going to be before any treatment is given. The ability to control the time the source spends in each dwell position allows for much greater target conformality and normal tissue sparing. |
Fig 2: These four images are used to evaluate the implant using the 3D CT based software. The upper left image shows the implant in 3D. The physician can rotate the implant to assess the radiation coverage by the prescription dose "cloud" from any angle, and the proximity of the implant to other structures, such as the rectum and bladder. Clockwise, three CT images show the radiation dose levels at the top, middle and bottom of the gland. | ||
 |
Fig 3: This close-up 3-D image of the 100% isodose cloud, showing near complete coverage of not only the prostate plus 5mm margin, but also the proximal seminal vesicles, shown semi-transparently. Notice how the dose cloud is shaped posteriorly to spare the anterior rectal wall. | ||
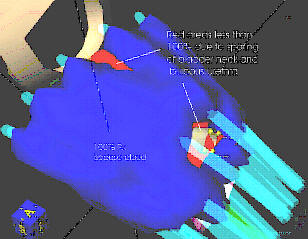 |
Fig 4: This view evaluates the implant from the top. The red areas are the small portions of the target volume that are spared the full prescription dose: the bladder neck and the lower bulbous urethra to prevent urinary incontinence and urethral stricture respectively. | ||
Back to TopDose Volume Histograms
Another way of evaluating the implant is to plot a dose volume histogram (DVH). A DVH tells the physician how much of the target volume is covered by the 100% prescription dose, and how much of the prescription dose the rectum and urethra receive. At CET, we routinely see 95% or higher, coverage to the target volume, which includes the proximal seminal vesicles and a 5mm margin around the prostate to include any extracapsular extension. The actual prostate receives 10% to 25% higher than the prescription dose. This results in a D90 (the dose 90% of the prostate volume receives) of 105 to 113% compared to most permanent seed implants which are considered 'optimal' if the D90 is 90%. |
Fig 5: This DVH shows that 97.4 % of the target volume is being encompassed by the prescription dose. 35% of the urethra received doses slightly higher than the prescription dose, with the maximum dose being around 110% of the prescription dose. The maximum anterior rectal wall dose our physicians allow is 75% of the prescription dose, versus up to 100% with seeds or external beam. | ||
Back to TopRadiograph Based Dosimetry
There are some instances where CT cannot be used to do the dose calculations. Hip prostheses cause artifacts in the CT images making the prostate and catheters hard to identify. Patients with severe claustrophobia have a problem being scanned. This technique, while not resulting in 3-D images, is a highly accurate technique that has been used for years before CT imaging became available. |
Fig 6: This is an "AP" (front view) radiograph of a CET prostate implant. The blue markings are the rectal outline and dose calculation points for the bladder, urethra and rectum. "Dummy" markers are inserted in the catheters. Contrast is introduced into the bladder (cystogram). Contrast is also used to inflate the foley balloons in the bladder and rectal catheters. The bladder catheter is made of a radio-opaque material to see the urethra clearly. Notice how the catheters can be made to flare in order to encompass any extracapsular extension. | ||
 |
Fig 7: This is a lateral (side view) of the CET prostate implant. The physicians try to lift the prostate away from the rectum to help achieve low rectal doses. Notice how the tips of the catheters are against the bladder. This ensures that any tumor in the base of the gland is adequately treated, yet by adjusting the time the source spends in the tip "dwell" positions, the bladder doses are controlled. | ||
Back to TopTypical CET HDR Dose Distributions
Fig 8: HDR Dose Dose Distributions
This is a transverse view of a typical CET prostate implant showing the radiation "isodose" levels. The red lines/dots are the superimposed dwell positions along the 17 catheters. (imagine looking end on at a string of beads). Notice the central area of reduced dose created by the ability to adjust the time the source spends in the 5 interior catheters to spare the urethra. The red line going around the implant is the prescription isodose line. Notice the space between the implant and the rectal points. In its natural position, the prostate lies on top of the
Back to TopTumor Specific Boosting
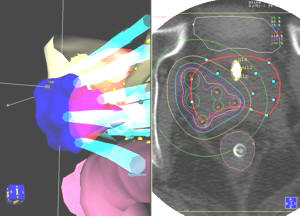 |
Fig 9: Specific Radiation Boosting: CET was the first center to realize and use the ability of the HDR system to send the source to specific positions in the catheters allowing us to give an additional "boost" dose to the cancer nodules. The image on the left shows the 3-D boosted area in blue at it extends out past and into the (red semi-transparent) prostate. The transverse view CT image with the isodose levels is on the right. | ||
Composite Dose Distribution
 |
Fig 10: Composite Dose Distribution | ||
| This is the resulting isodose pattern of the initial whole gland plan combined with the boost, which we call the composite plan. The numbers are the isodose values in cGy (HDR). The highest dose areas are in the peripheral zone of the prostate, where most prostate tumors arise. Notice the larger boosted area that is covered by the 900 cGy (HDR) isodose line. The prescription dose, 600 cGy (HDR), is the inner red line going around the prostate. Note that the 600 cGy prescription is occurring 5mm out from the prostate capsule. If necessary, we can create an | |||
Back to TopExample of HDR Conformity and Accuracy: Sparing a TURP defect
A common procedure done to relieve pressure of an enlarged prostate on the urethra is called a transurethral resection of the prostate (TURP). An incision is made in the urethra and part of the urethra and prostate tissue is removed. Some men experience some incontinence after this procedure. In order to avoid exacerbating this situation, we spare the TURP defect as much as possible by limiting the radiation dose to less than 105% of the prescription dose. We have found that this dose is tolerated by the urethra while still delivering the necessary tumoricidal dose to the prostate.The HDR system allows for much greater conformality than permanent seeds. With seeds, one hopes that they don't move near or into the defect and the dose to the defect is not known after the one month post-implant dosimetry is done. With HDR, we can accurately shape the radiation dose to avoid the defect while knowing what the doses will be before any treatment is given.
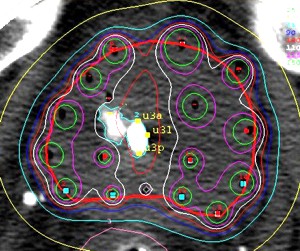 |
Fig 11: HDR Conformity and Accuracy Sparing a TURP defect: This image shows how we can accurately shape the radiation dose (white line) to go around the contrast-filled TURP defect. This precision is not possible with EBRT or permanent seeds. | ||
Back to Top3. Permanent Seed or LDR Brachytherapy
Permanent seed implants are a form of interstitial, Low Dose Rate (LDR) brachytherapy. Iodine-125 and Palladium-103 are the two radio-isotopes used in seed implants. In general, brachytherapists choose isotope for treatment based on the aggressiveness of the tumor. Iodine-125 has a slower dose rate and is used on slower growing tumors, where as, Palladium-103 has a higher dose rate and is used on faster growing tumors. This selection method has not been verified in any formal studies as an effective method. Implant isotope seed is tiny, 1mm x 5 mm in size. They are permanently inserted into the prostate and left there to radioactively decay.Permanent seed implants alone (monotherapy) are used to treat prostate cancer which has a high probability of being confined to the prostate.
Back to TopThe criteria for permanent seed monotherapy are:
- Stage T1-T2a
- Prostate volume < 60 cc at time of implant
- PSA<10
- Gleason score < 6
- No significant obstructive symptoms
- No perineural or extracapsular extension
- < 3 of 6 sextant biopsies positive
Back to TopProcedure for Permanent Seed Brachytherapy
Prior to the permanent seed implant, a trans-rectal ultrasound examination is done to determine the shape and size of the prostate. The prostate is "mapped" on a square grid template and a pre-plan calculation is done to determine which holes in the template the needles need to be inserted and how many seeds to deposit through each needle in order to adequately irradiate the prostate.In the operating room, the patient is placed under general or spinal anesthesia. The ultrasound probe, rather than being able to be maneuvered free-hand as in the non-fixed technique, is attached to the "stepper" assembly that also holds the square grid template against the perineum. The physician pushes stainless steel needles through the pre-determined holes in the template, into the perineum and then the prostate, guided by the images seen on the ultrasound. After each needle is in the proper position, the seeds are inserted, according to the pre-plan dosimetry. The physician can modify the seed placement from the pre-plan based on skill and experience. For example, the physician may decide to place additional seeds in areas of the gland that look to be potential "cold" spots. Once a seed is deposited, nothing that can be done to change its position. Physician experience is paramount in doing a successful seed implant.
The number of seeds used depends on the size of the prostate. Most prostate implants require 60 to 120 seeds. With the insertion of the seeds, the patient is now radioactive. Radiation safety precautions are followed to minimize the radiation exposure to hospital staff and family members. It is recommended that pregnant women, and children should avoid close contact with the patient for about two months, until the sources have decayed to a lower level of radioactivity.
Some seeds may migrate out of the implant. They have appeared in the urine, in the ejaculate, and in the lungs of some patients. It is not necessary to retrieve the seeds that are passed in the urine. Before engaging in sex, men should use a condom to catch any seeds that may be in the ejaculate. Any seed loss should be reported to the radiation oncologist. To date, there is no evidence of any ill-effects caused by seed migration to the lungs.
After one month, a CT scan and special x-ray films are done in order to do the final "post plan" calculation to determine what radiation doses the prostate and surrounding organs actually received due to the shifting and migration of the seeds. A chest x-ray is done to see if any seeds migrated into the lungs.
Back to Top4. Comparing HDR and Permanent Seed
The following table was compiled by the HDR Prostate Working Group and presented to radiation oncologists at the American Society of Therapeutic Radiology and Oncology (ASTRO) meeting in Phoenix, October 1998. Comparison of High Dose Rate Temporary Implants and Permanent Seed Implants
Treatment attributes |
High Dose Rate |
Permanent Seed |
| Conformal treatment | ++++ | +++ |
| Target accuracy | ++++ | +++ |
| Ability to treat extracapsular extension | ++++ | + |
| Ability to treat seminal vesicles | ++++ | ++ |
| Ease of control of radiation | ++++ | ++ |
| Lack of cold/hot spots | ++++ | ++ |
| Control of critical organ dose | ++++ | ++ |
| Modify dose distribution | ++++ | + |
| Need for external beam | Yes, at present* | Sometimes |
| Monotherapy | *** | +++ |
| Experience of Physician | Crucial | Crucial |
| Pre-planning dosimetry | not needed | Extensive (TRUS) |
| Post implant dosimetry | not needed | Extensive (CT) |
| Stages treated | All, T1-T3 | T1-T2 |
| Gland volume>60 ccat time of implant | less difficulty | more difficulty |
| Pubic Arch interferenceat time of implant | less of a problem | can't be done |
| Prior TURP | less of a problem | can't always be done |
| Final Dose Verification | pre-treatment | post treatment |
| Symptom duration | weeks | months |
| Implant cost | comparable | comparable |
Our physicians disagreed with the authors of the above chart who said that EBRT is necessary with HDR. Our physicians reasoned that if permanent seeds can be used as a monotherapy treatment for low risk disease (T1 - T2a), then so can HDR. In 1996, we began our Monotherapy Program. A select group of patients are eligible for HDR monotherapy if they meet the following criteria:
- Clinical stage T1a - T2a (possible T2b)
- Gleason score 7(must be 3 + 4, not 4 +3 ) or less
- PSA 10 or less
- 50% or less of the biopsy cores positive
Back to Top5. Consideration for Choosing HDR
- There are no seeds to migrate into the bladder, rectum, urethra, seminal vesicles or lungs
- Radiation exposure to others is eliminated
- Dose accuracy and control is much higher than with seeds
- The doses to other structures are known before any treatment is given
- Pubic arch interference is much less of a concern, so pre-treatment hormones, and their side effects, are avoided
- Post implant morbidity (side effects) is less and of shorter duration than with seeds
- Post implant costs are less with HDR due to the lessened use of medications and very rarely needed catheterization.
Home
Our Treatment Programs
- Prostate Cancer

 Monotherapy Survival Rate
Monotherapy Survival Rate- Vaginal Cancer
- Cervical Cancer
- Endometrial Cancer
- Vulvar cancer
- Breast Cancer
- Head and Neck Cancer
- Lung Cancer
- Esophageal and Bile Duct Cancer
- Soft Tissue Sarcoma Cancer
Our Treatments Statistics
Frequently Ask Questions
General Information
Our Publications
Cancer Resources & Links
Back to TopGeneral Frequently Asked Questions
1. How does radiation kill cancer?
Cancer is made of abnormal cells that tend to grow without control. Cancer DNA is more sensitive to radiation than are normal cells, so radiation kills cancer directly or when the cells attempt to multiply while normal tissue in the region is able to repair and recover.
2. What is Brachytherapy?
The prefix "brachy" is the Greek word for "short" distance. Brachytherapy is a form of internal radiation treatment where radioactive sources are placed on or into cancer tissues. There are two kinds of brachytherapy. The radiation sources may be inserted either permanently or temporarily. The two most common forms of treatment are low dose rate (LDR) permanent seeds for prostate cancer and high dose rate (HDR) temporary brachytherapy, that can be used for prostate, gynecologic, breast, head and neck, lung, esophageal, bile duct, anorectal, sarcoma, and other cancers.
3. What is high dose rate (HDR) Brachytherapy?
High dose rate (HDR) is a technically advanced form of brachytherapy. A high intensity radiation source is delivered with millimeter precision under computer guidance directly into the tumor killing it from the inside out while avoiding injury to surrounding normal healthy tissue. For a more in depth explanation please go to understanding HDR Brachytherapy page.
4. What are the advantages of HDR Brachytherapy?
- Preservation of organ structure and function
- Improved accuracy and precision of radiation dose delivery
- Knowledge of radiation dose distribution before treatment is given
- Ability to shape the radiation dose to fit the tumor
- Fewer side effects
- No radiation source (seeds) migration into other organs
- No radiation exposure to other persons
- The treatment course is days rather than weeks to months (as required for permanent seeds or external beam)
- Excellent coverage of possible microscopic extension of cancer
- Minimizes areas of radiation overdose (hot spots) or underdose (cold spots)
- Organ motion (target movement) is not a problem for HDR as it is with external beam
- Effective treatment for cancer recurrence (termed "salvage" therapy)
5. How successful is HDR Brachytherapy?
HDR Brachytherapy is proven to be effective for the treatment of local disease in many forms of cancer including prostate, gynecological, breast, head and neck, esophagus, lung, anorectal, bile duct, sarcoma, and other primary cancer or localized metastasis as reported in the medical literature. CET's publication on prostate cancer, for example has demonstrated 90% 10-year tumor control. Success rates for other tumors vary according to the type and stage of cancer being treated.
6. How many treatments has CET administered?
As of 8/31/2005, CET has performed 8,023 HDR implants and delivered 16,464 HDR treatments. Please see our treatment statistics for further details.
7. Why is HDR less well known than other forms of cancer treatment?
HDR Brachytherapy is a relatively new form of advance radiation technology. Fewer physicians have been trained to perform HDR procedures compared to seed implants or external beam radiation. Few centers, other than CET have been dedicated to the development of HDR brachytherapy to its full potential. Dr. Demanes has devoted his career to the advancement of brachytherapy and has pioneered the use of HDR and established CET as a center of excellence with specially trained and experienced staff and physicians.
8. Why should I select CET?
- Most experienced HDR center in the country
- First center specializing solely in HDR brachytherapy
- Recognized as HDR experts by colleagues in radiation oncology
- Acknowledged safety record
- Highly trained and experienced physicians and staff
- Long term results published in peer reviewed medical literature
- Quality patient care and follow up
Back to TopAbout Us
-
California Endocurietherapy Cancer Center (CET) is the first brachytherapy only center in the United States.
-
Founded by D Jeffrey Demanes M.D. in 1981.
-
Dedicated solely to High Dose Rate brachytherapy (HDR) since 1991.
-
Most experienced HDR brachytherapy center.
-
A training destination for physicians and residents.
-
HDR treatment protocol development
-
Innovation in high dose rate brachytherapy and equipment design
-
Dedicated to long-term follow-up, outcome studies, and publications in medical journals.
Membership and affiliations
 |
American Society for Therapeutic Radiology And Oncology Chair - Health Policy and Economics Practice Management Subcommittee, Chair - Regulatory Subcommittee, Member - Health Policy and Economic Committee, Member - Health Policy and Economics Code Development and Valuation Subcommittee, Member - Code Utilization and Application Subcommittee. |
 |
|
 |
American College of Radiation Oncology President - 2005 to 2006 |
Back to Top
CET Cancer Center
California Endocurietherapy Medical Corp.3012 Summit St. Suite 2675, Oakland, CA 94609
Tel: 877-238-1437 or 510-986-0690 Fax: 510-986-0159
Hours: Mon-Fri, 8:30AM to 5:00PM Pacific Time
Copyright California Endocurietherapy Medical Corp. All Rights Reserved. www.cetmc.com