 |
310-206-2510
|
Gynecologic Brachytherapy
(High Dose Rate Brachytherapy for Cervical Cancer, Endometrial Cancer, Vaginal Cancer, Vulvar Cancer)
Back to Top1. Introduction
Brachytherapy plays a central role in the treatment of gynecologic cancers. Some treatment protocols require part of the radiation dose be delivered by brachytherapy. Early stage tumors may be treated with intracavitary implants. More extensive tumors require interstitial implants. Definitive treatment with radiation therapy involves a combination of external beam radiation therapy plus brachytherapy.
At CET, we favor high dose rate (HDR) brachytherapy. With HDR, the radioactive source delivers the prescribed radiation dose in a matter of minutes. This eliminates the lengthy, uncomfortable hospital stay of at least two days which is required if low dose rate brachytherapy is used
Back to TopTable of Contents
Back to Top2. Intracavitary Implants
Intracavitary implants differ by the type of applicator used. The applicators are specially designed to deliver the radiation according to the tumor site. Patients treated with intracavitary applicators receive 3 to 6 treatments, delivered on an out-patient basis.Preparation for Intracavitary Implants
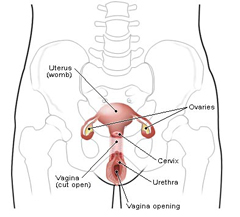
On the evening before an applicator insertion, the patient is requested to have a light dinner (broth, jello) and not to eat or drink after midnight. A little water is permissible to take medications. The patient performs a Fleet enema the night before and the morning of the insertion. At the clinic, the patient lies supine (on the back) on the padded treatment couch in the treatment position with feet in stirrups. The nurse will administer conscious sedation to relax the patient, if necessary. Local anesthetic may also be given at the beginning of the insertion. The nurses gently wash the perineal and genital area. Sterile drapes are placed around the vaginal area. Catheters are inserted into the bladder and rectum for the introduction of contrast liquid. This contrast is necessary to visualize the bladder and rectum on radiographs so that radiation doses to these structures can be calculated.CET Offers 2 Types of Intracavitary Implants
Back to Top2.1 CET's Multichannel Vaginal Cylinder
Fig 1: CET's Multichannel Vaginal Cylinder Applicator Setup
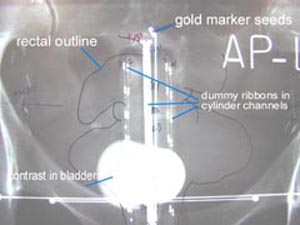 |
Postoperative brachytherapy may be needed following a hysterectomy for endometrial (uterine) cancer. Treatment is delivered with brachytherapy to the upper vaginal area, an area at high risk for recurrence. The CET vaginal cylinder is a smooth, plastic cylinder, measuring a little over 1 inch in diameter. It has 7 channels through which the radioactive source can travel. The multichannel cylinder allows for greater dose control and radiation dose shaping than the central channel only cylinder. CET published a study (The Use and Advantages of a Multichannel Vaginal |
Back to Top2.2 CET's Demanes-Rodriguez Tandem and Ovoids Applicator
Fig 2 : Demanes-Rodriguez Tandem and Ovoids Applicator Setup
 |
Brachytherapy for early stage cervix cancer is delivered using an applicator called a tandem and ovoids. Prior to the first treatment is the intraoperative placement of a Smitt sleeve. The Smitt sleeve is a hollow plastic tube, custom fitted to the uterine cavity. It is inserted through the cervical opening into the uterus then sutured in place onto the cervix. This sleeve stays in the uterus for the duration of the treatments. The purpose of the Smitt sleeve is to keep the cervix open which |
Back to Top3. Interstitial Implants
Fig 3: Interstitial Implants: dummy radiation source appears as a dotted line.
 |
Interstitial implants are required for more advanced stage gynecologic malignancies. Generally, two implants are performed, a week apart, with each implant receiving two to three HDR treatments. The implants are done under spinal anesthesia in the operating room. Hollow plastic catheters are inserted through the perineum, guided with ultrasound, fluoroscopy and endoscopy, to fully encompass the tumor. |
Back to Top4. Consideration
High dose rate brachytherapy allows precise delivery of the radiation dose prescribed by the physician. The ability to shape the radiation doses to maximize tumor dose and minimize dose to surrounding normal tissues is a great advantage over low dose rate methods and excellent tumor control rates and low side effect rates are being realized in our clinic. The short treatment times, outpatient visits, and accurate radiation delivery are all advantages of the HDR system.
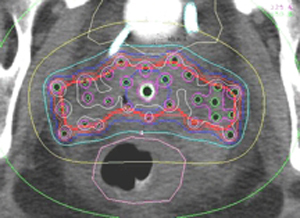
Fig 4: CT Dosimetry:This is a transverse view of an interstitial implant for cervical cancer that has extended beyond the "reach" of the tandem and ovoids applicator. Note how the radiation dose can be adjusted to avoid overdosing the rectum and bladder. The physicians also placed treatment catheters to treat the pelvic lymph nodes.
Home
Treatment Programs
- Prostate Cancer

 Monotherapy Survival Rate
Monotherapy Survival Rate- Breast Cancer
- Vaginal Cancer
- Cervical Cancer
- Endometrial Cancer
- Vulvar cancer
- Head and Neck Cancer
- Lung Cancer
- Esophageal Cancer
- Bile Duct Cancer
- Soft Tissue Sarcoma Cancer
Treatments Statistics
Glossary
Frequently Ask Questions
General Information
Brachytherapy Publications
Cancer Resources & Links
Back to TopGeneral Frequently Asked Questions
1. What is Brachytherapy?
The prefix "brachy" is the Greek word for "short" distance. Brachytherapy is a form of internal radiation treatment where radioactive sources are placed on or into cancer tissues. There are two kinds of brachytherapy. The radiation sources may be inserted either permanently or temporarily. The two most common forms of treatment are low dose rate (LDR) permanent seeds for prostate cancer and high dose rate (HDR) temporary brachytherapy, that can be used for prostate, gynecologic, breast, head and neck, lung, esophageal, bile duct, anorectal, sarcoma, and other cancers.
2. What is high dose rate (HDR) Brachytherapy?
High dose rate (HDR) is a technically advanced form of brachytherapy. A high intensity radiation source is delivered with millimeter precision under computer guidance directly into the tumor killing it from the inside out while avoiding injury to surrounding normal healthy tissue. For a more in depth explanation please visit the understanding HDR Brachytherapy page.
3. How does radiation kill cancer?
Cancer is made of abnormal cells that tend to grow without control. Cancer DNA is more sensitive to radiation than are normal cells, so radiation kills cancer directly or when the cells attempt to multiply while normal tissue in the region is able to repair and recover.
4. What are the advantages of HDR Brachytherapy?
- Short course of treatment compared to other types of radiation treatment (1 week)
- Preservation of organ structure and function
- Fewer side effects
- Excellent coverage of possible microscopic extension of cancer
- Knowledge of radiation dose distribution before treatment is given
- Accuracy and precision of tumor specific radiation dose delivery
- Minimizes areas of radiation overdose (hot spots) or underdose (cold spots)
- Organ motion (target movement) is not a problem for HDR as it is with external beam
| Prostate Specific |
- Effective treatment for cancer recurrence (termed "salvage" therapy)
- No radiation source (seeds) migration into other organs
- No radiation exposure to other persons
| Breast Specific |
- Conserves the breast and yields excellent cosmetic results
- Reduces radiation dose to the heart, lungs, and opposite breast
- Doesn't cause a delay in other treatments such as chemotherapy
For more information on the advantages for specific cancer sites please click on the appropriate link below:
Prostate cancer | Breast Cancer | Gynecologic Cancer | Head & Neck Cancer
Esophageal and Bile Duct Cancer | Lung Cancer | Soft Tissue Sarcoma Cancer
5. How successful is HDR Brachytherapy?
HDR Brachytherapy is effective treatment of local disease in many forms of cancer including prostate, gynecological, breast, head and neck, esophagus, lung, anorectal, bile duct, sarcoma, and other primary cancer or localized metastasis as reported in medical literature. CET's publication on prostate cancer, for example has demonstrated 90% 10-year tumor control. Success rates for other tumors vary according to the type and stage of cancer being treated.
6. How many treatments has CET administered?
As of 12/31/2009, CET has performed 10,267 HDR implants and delivered 21,878 HDR treatments. Please see our treatment statistics for further details.
7. Why is HDR less well known than other forms of cancer treatment?
HDR Brachytherapy is a relatively new form of advance radiation technology. Fewer physicians have been trained to perform HDR procedures compared to seed implants or external beam radiation. Few centers, other than CET have been dedicated to the development of HDR brachytherapy to its full potential. Dr. Demanes has devoted his career to the advancement of brachytherapy and has pioneered the use of HDR and established CET as a center of excellence with specially trained and experienced staff and physicians.
8. Why should I select CET?
- Most experienced HDR center in the country
- First center specializing solely in HDR brachytherapy
- Recognized as HDR experts by colleagues in radiation oncology
- Acknowledged safety record
- Highly trained and experienced physicians and staff
- Long term results published in peer reviewed medical literature
- Quality patient care and follow up
Back to TopAbout Us
-
California Endocurietherapy Cancer Center (CET) is the first brachytherapy only center in the United States.
-
Founded by D Jeffrey Demanes M.D. in 1981.
-
Dedicated solely to High Dose Rate brachytherapy (HDR) since 1991.
-
Most experienced HDR brachytherapy center.
-
A training destination for physicians and residents.
-
HDR treatment protocol development
-
Innovation in high dose rate brachytherapy and equipment design
-
Dedicated to long-term follow-up, outcome studies, and publications in medical journals.
Membership and affiliations
 |
 |
 |
| American Society for Therapeutic Radiology And Oncology Chair - Health Policy and Economics Practice Management Subcommittee, Chair - Regulatory Subcommittee, Member - Health Policy and Economic Committee, Member - Health Policy and Economics Code Development and Valuation Subcommittee, Member - Code Utilization and Application Subcommittee. American Brachytherapy Society Chair - Socioeconomic Committee. American College of Radiation Oncology President - 2005 to 2007 American College of Radiology Fellow - 2007 |
Back to Top
CALIFORNIA ENDOCURIETHERAPY AT UCLA
Division of BrachytherapyDepartment of Radiation Oncology
200 UCLA Medical Plaza, Suite B265
Los Angeles, CA 90095-6951
Tel: 310-206-2510 Fax: 310-794-9795
Hours: Mon-Fri, 8:30AM to 5:00PM Pacific Time
Copyright California Endocurietherapy Medical Corp. All Rights Reserved. www.cetcancercenter.com